Where Interpersonal Theory Meets the Inner World
Using CIIT to guide evidence-based psychodynamic work with borderline patients.


You are twelve minutes into a session. Your patient, who has been doing better for weeks, arrived late, won’t make eye contact, and just told you with a shrug that she cut herself last night after her boyfriend mentioned he had weekend plans. She is oscillating between “I don’t even care about him” and barely suppressed tears. You can feel the pull in your own body: the urge to lean in, to work harder, to prove you are not the indifferent other she seems to be bracing for. You know that urge is important, that it is telling you something about what is happening between the two of you right now, but you are not sure what to do with it.
This is the territory where most clinical writing fails. It gives you frameworks for understanding personality disorder in the abstract but leaves you alone in the room with a patient whose pain is organized in a way that makes your next move matter enormously and your ability to think about it feel compromised.
This post is about what happens when three well-researched approaches to personality disorder are brought together in moments like this one. The three are Contemporary Integrative Interpersonal Theory (CIIT), Mentalization-Based Treatment (MBT), and Transference-Focused Psychotherapy (TFP). Each sees something the others don’t. Together, they give clinicians something closer to a complete picture of what is going on and what to do about it.
We will return to the session described above. But first, a brief look at what each model contributes and why the integration is not as seamless as it might appear.
The Interpersonal Situation: A Map You Already Use
CIIT is built on an observation that most therapists already know intuitively: the most important things in a person’s life happen in the space between them and other people. Not inside a single mind in isolation, but in relationships. What a person wants from others, how they read others’ intentions, what they feel in response, and what they actually do. These four systems (motivation, perception, affect, behavior) interact dynamically. In healthy functioning, they are coordinated. In borderline personality disorder, they are not.
If you have ever noticed that a patient seems to perceive hostility that you did not intend, and that this misperception triggers shame, which activates a self-protective withdrawal, which then creates the very distance the patient feared in the first place, you have already been thinking in CIIT terms.
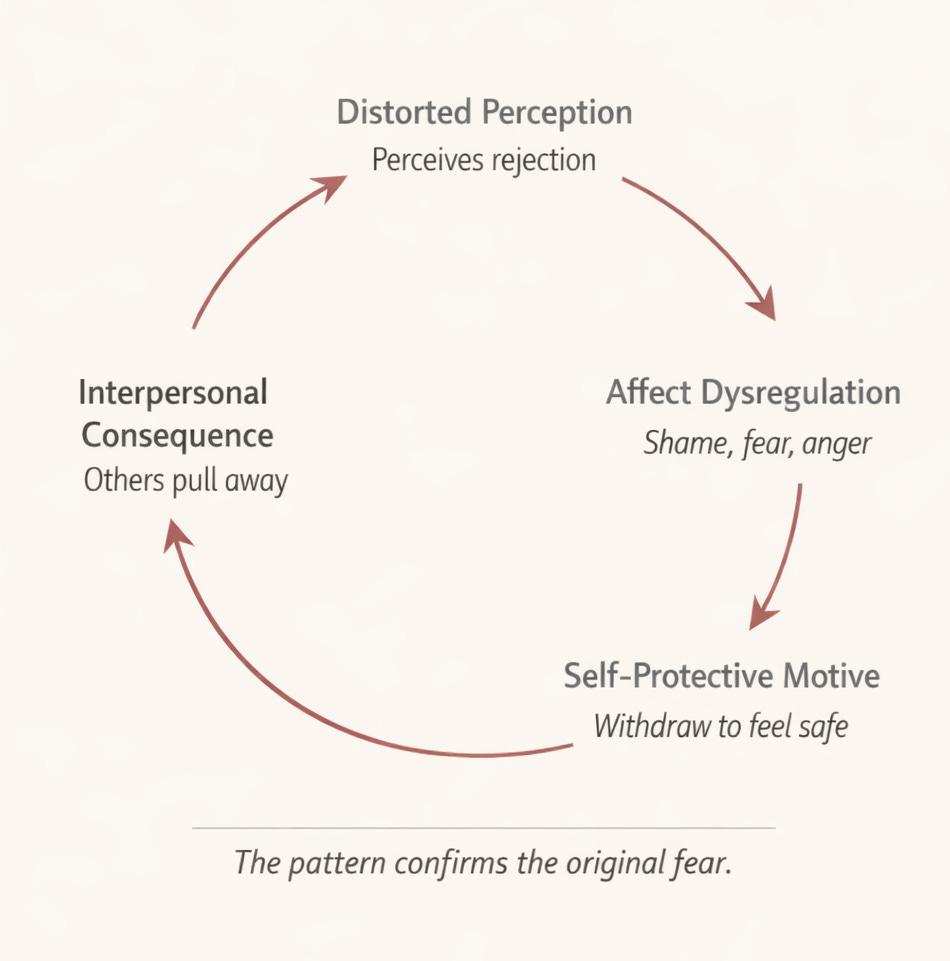
The framework calls this a vicious circle driven by parataxic distortion (Sullivan’s term for the way internalized relationship templates distort the perception of current interactions) and self-protective motives (rigid or chaotic efforts to restore felt security when it feels threatened).
CIIT organizes interpersonal behavior along two dimensions that decades of research have validated: agency (dominant to submissive) and communion (warm to cold). This gives clinicians a precise, shared language for tracking what is happening moment to moment: “She just shifted from warm and open to cold and withdrawn. What triggered that shift? What is she protecting herself from?”
The crucial point is that CIIT is not a new school of therapy. It does not ask clinicians to abandon their existing training. It is, in its own language, not “interpersonal therapy” but “therapy conceptualized interpersonally.” Whatever you already do, whether that is transference interpretation, cognitive restructuring, behavioral activation, or acceptance work, can be understood and refined through this lens. CIIT holds other models rather than competing with them.
Two intervention principles make this holding possible. Strategic complementarity means deliberately choosing how to respond to the patient’s interpersonal pull, sometimes matching it, sometimes disrupting it. Therapeutic metacommunication means stepping back to name the interpersonal process unfolding between patient and therapist in real time. Metacommunication can be implemented through many specific techniques, from mentalizing interventions to transference interpretations. The framework accommodates both.
MBT: When Thinking About Minds Breaks Down
MBT focuses on mentalizing: the ability to understand your own and others’ behavior in terms of underlying thoughts, feelings, wishes, and intentions. It sounds basic, but it is actually fragile. We all lose it under stress. People with BPD lose it precisely when it matters most, in emotionally charged relationships where closeness, rejection, or loss feels at stake.
When mentalizing collapses, MBT describes three characteristic modes. In psychic equivalence, feelings become facts: “He doesn’t care about me” is not a worry but an unshakeable certainty. In teleological thinking, only visible, physical proof counts: words of reassurance mean nothing without concrete action. In pretend mode, a person can talk about feelings at length but in a disconnected, intellectual way that never touches real emotion.
The MBT therapist’s job is to notice when mentalizing has collapsed and help bring it back. The sequence is deliberate: validate the patient’s emotional experience first (lowering the temperature enough that thinking can resume), then help the patient name and explore their feelings with more specificity, then identify the interpersonal dynamic playing out between patient and therapist in the session itself. This last step, mentalizing the therapeutic relationship, is the training ground for learning to stay reflective inside emotionally charged interactions everywhere else.
TFP: The Fractured Inner World
TFP comes from a psychodynamic object relations tradition and sees borderline pathology differently. Its core idea is that people with BPD suffer from identity diffusion: their inner world is populated by extreme, contradictory images of self and other that cannot be held together at the same time.
We all have mixed feelings about important people. A parent can be both loving and frustrating. Normally, we hold these contradictions together. In BPD, the integration has not been achieved. Instead, the inner world is organized into separate, opposing pairs: a helpless self paired with a cruel other, a special self paired with an ideal caretaker. These pairs alternate rapidly but are never experienced simultaneously. TFP calls this splitting. It shows up in therapy as dramatic oscillation, idealization one week, devaluation the next, and the therapist’s countertransference (feeling wonderful, then feeling useless) is often the clearest signal that it is happening.
TFP works by helping the patient gradually become aware of these opposing images and, over time, integrate them. The therapist clarifies what the patient is experiencing (which is often unclear even to the patient), confronts contradictions the patient has not noticed, and interprets why the patient needs to keep these images separate and what it might mean to bring them together.
The Tension Between Models
It would be dishonest to suggest that MBT and TFP slot together without friction. They don’t.
MBT is deliberately non-interpretive. Its stance is one of “not-knowing.” The clinician avoids claiming to understand the patient’s unconscious motivations because doing so risks taking over the patient’s own mentalizing. The MBT therapist does not say “You are projecting your anger onto me.” The MBT therapist says “I wonder what’s happening between us right now.” The distinction matters: one names the process from the outside, the other invites the patient to discover it from the inside.
TFP, by contrast, is explicitly interpretive. The therapist formulates a hypothesis about the object relations dyad being enacted in the transference and presents it to the patient, often with conviction, because the patient’s primitive defenses will resist anything that feels tentative. “You seem to be experiencing me as a harsh critic right now, and I think that is protecting you from a wish to depend on me that feels too frightening.” That is a TFP-style interpretation. An MBT clinician would approach the same moment very differently.
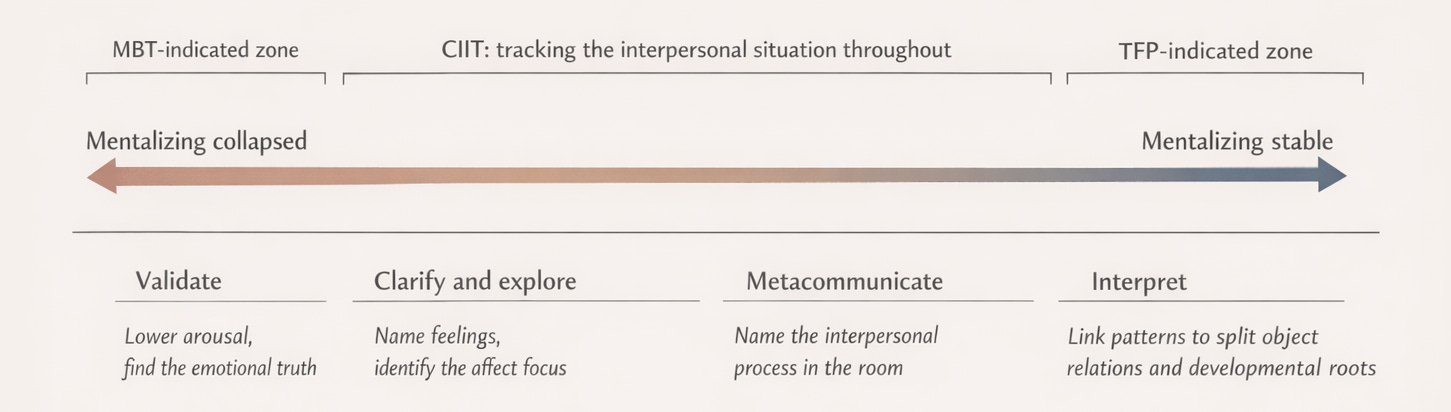
This is a real tension, not a superficial one. The question is: can a clinician know when to use which? CIIT’s answer is yes, because the interpersonal situation tells you what the patient needs at a given moment. When mentalizing has collapsed and the patient is in psychic equivalence, an interpretation will not land. It will be experienced as the therapist imposing their reality onto the patient’s, which is exactly the kind of interaction that reinforces the problem. In that moment, the MBT approach is indicated: slow down, validate, bring mentalizing back online. When mentalizing is more stable and the patient has some observing distance, interpretation becomes possible and even powerful. The patient can hold the therapist’s hypothesis alongside their own experience without feeling invaded by it.
CIIT does not erase the tension between these models. But it gives clinicians a principled basis for navigating it.
The Session

Back to the room. The patient’s name is Nadia. She is 31, and she has been in therapy for five months.
Nadia grew up with a mother who was warm and effusive when things were good but who would turn cold and punishing without warning, often for reasons Nadia could never understand. Her father was largely absent. The unspoken family rule was that closeness was conditional and could be revoked at any time. Nadia internalized this. She oscillates between warmth and sharp hostility with the people she is closest to, reenacting her mother’s unpredictability without realizing it. She reads every interaction for signs that the other person is about to withdraw, as though her mother’s cold turn is always imminent. And she treats herself with contempt when things go wrong, having internalized the message that she is the cause of others’ rejection.
Today, Marcus mentioned weekend plans. By the time Nadia went to bed, she had sent him a string of accusatory texts and scratched her forearms with a broken pen cap. She arrives at session late, arms crossed, alternating between “it’s not a big deal” and visible despair.
Dr. Reyes, her therapist, begins by tracking the interpersonal situation. On the surface, Nadia is cold and dismissive, pushing her away. But the tears breaking through tell a different story. Underneath the bravado, Nadia is likely experiencing herself as abandoned and helpless, with Marcus and perhaps Dr. Reyes cast as indifferent. The dismissiveness is a self-protective reversal: Nadia is trying to regain control by becoming the one who doesn’t care. But the two experiences, the dismissive Nadia and the devastated Nadia, are not connected. She cannot hold them at the same time.
Dr. Reyes knows that Nadia’s mentalizing has collapsed. Nadia is in psychic equivalence: “Marcus is leaving me” has become an unquestionable fact. Challenging it directly would only escalate things. So Dr. Reyes starts with empathic validation: “It sounds like last night was really painful, even if it doesn’t feel safe to say that right now.”
Nadia shrugs. Her eyes fill. Something shifts. Dr. Reyes notices her own internal pull: the urge to work harder, to be warmer. She recognizes this as clinical data. Nadia may be unconsciously casting her in the role of the needed-but-unreliable caretaker, the same role Marcus occupies, the same role her mother occupied.
With Nadia slightly more settled, Dr. Reyes names what she sees: “I notice something happening between us today. You came in late, and you’re keeping me at a distance. I don’t think that’s random. I wonder if part of what happened last night with Marcus is also happening here. When someone matters to you and they do something that feels like pulling away, you protect yourself by pulling away first.”
This is metacommunication in CIIT’s terms. It is also, in this moment, a transference interpretation, and it works because Nadia’s mentalizing has recovered enough to hold it. The intervention names the pattern: the terrified, attached self and the indifferent other, linked by fear of abandonment. It names the self-protective reversal. And it draws a line between the therapy relationship and the outside relationship.
Nadia is quiet. Then: “I just don’t understand why everyone leaves.”
A shift, but from one extreme to another. She has dropped the bravado but moved into global despair. She is still not holding both experiences together. Dr. Reyes stays with the process rather than the content.
“You’ve described how your mother could be completely with you one moment and then turn on you the next. I think that experience taught you something. It taught you that closeness is dangerous because it can be revoked without warning. So when Marcus said he had plans, it wasn’t just about the weekend. Your whole system went on alert: this is the moment where they leave. And you acted on that alarm before you had a chance to check whether it was accurate.”
“I know I overreacted. I always overreact.”
Dr. Reyes resists the urge to reassure. Reassurance here would cast her as the good rescuer and Nadia as the bad patient, which is just another version of the split. Instead: “I’m less interested in whether you overreacted than in what it felt like before you sent those texts. You went from having a good thing with Marcus to being certain it was over. That’s a huge leap, and it happened in seconds. That leap is the thing worth understanding.”
Nadia pauses. “I think... I was fine when he first told me. I even said ‘have fun.’ But then when I was alone, it was like something switched. I kept picturing him having a great time without me and not thinking about me at all. And then it was like he didn’t care. And then I just felt nothing. Empty. And I couldn’t stand it.”
“So there were actually two Nadias last night. One who could hear that Marcus had plans and feel okay about it. And another who could not tolerate being alone with the thought that she might not be on his mind.”
Nadia looks up. “Yeah. That’s exactly it.”
For a moment, she is holding both. Not fused with either one. Not dismissing the pain and not drowning in it. Looking at it. Her mentalizing has recovered. The split images of self are, briefly, in the same room together. The vicious circle that runs from perceived rejection to hostile withdrawal to actual disconnection has been interrupted.
What Made This Possible
Not a single technique. A sequence of choices, each informed by a different model.
CIIT gave Dr. Reyes a way to track the interpersonal situation in real time: what Nadia was perceiving, feeling, wanting, and doing, and how those systems were interacting with each other and with Dr. Reyes’s own responses. MBT told her when to slow down (Nadia’s mentalizing had collapsed and needed to be restored before anything deeper could land) and what to do first (validate, lower arousal, rekindle reflective capacity). TFP told her what to name once the moment was right: the split images of self and other, the defensive function of the splitting, and the developmental roots of the pattern in Nadia’s relationship with her mother.
And the tension between MBT’s not-knowing stance and TFP’s interpretive conviction was not a problem to be resolved in the abstract. It was navigated in real time, session by session, moment by moment, guided by what Nadia could actually use at each point.
The moment Nadia looked up and said “Yeah, that’s exactly it” was not the product of a framework. It was the product of a therapist who could see clearly enough to resist her own pull to react, who could hold the complexity of what was happening without collapsing it into a single explanation, and who could sit with the uncertainty long enough for something new to emerge. The frameworks helped her do that. The rest was the work.